Why RTM Codes Get Generated But Never Get Paid
Why RTM Codes Get Generated But Never Get Paid
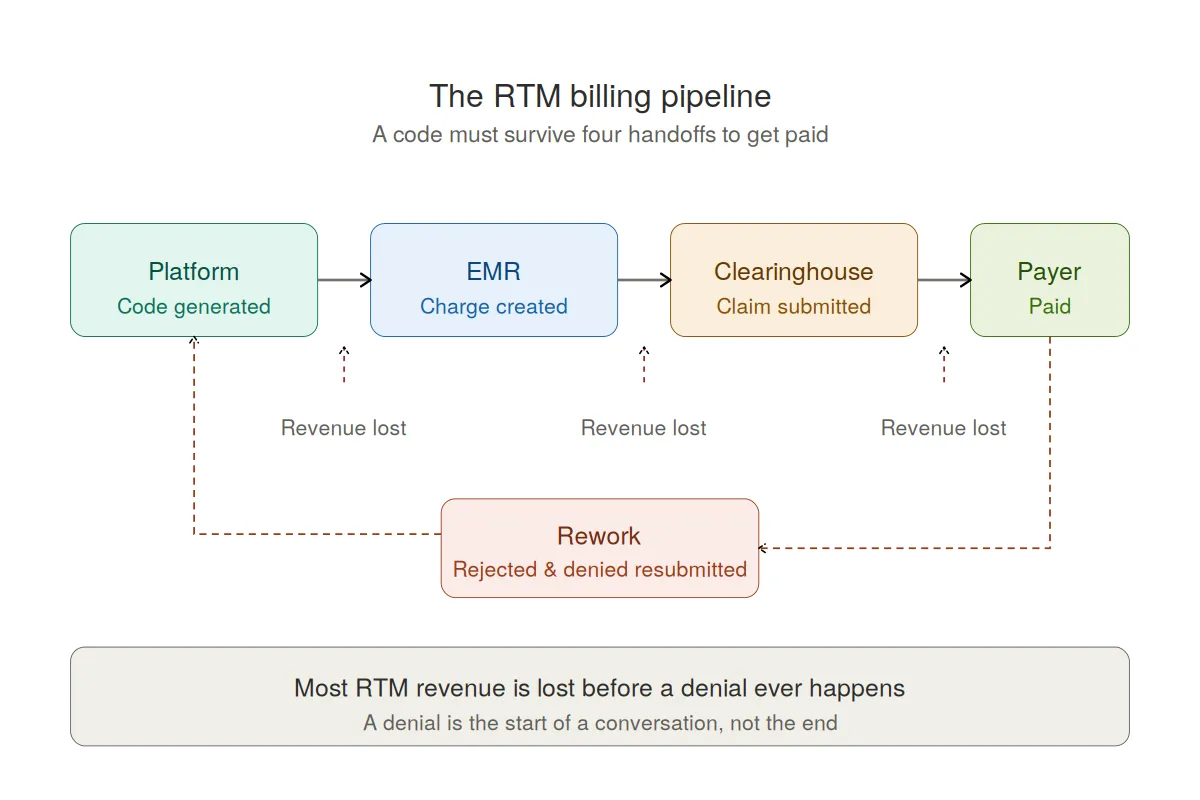
Most physical therapy practices lose RTM revenue not to payer denials, but to the handoffs between systems — the RTM platform, the EMR, the clearinghouse, and the payer. A code can be perfectly earned and perfectly documented and still never get paid because it falls through one of those four gaps before a claim is ever adjudicated.
This guide breaks down exactly where Remote Therapeutic Monitoring (RTM) billing leaks, why those leaks are nearly invisible, and how to close them across the full 2026 code set.
Where Does RTM Billing Actually Break Down?
RTM billing breaks down at four system handoffs, in this order: platform to EMR, EMR to clearinghouse, clearinghouse to payer, and finally payer adjudication. Codes are earned correctly inside the RTM platform and then drop out silently at each boundary, so most lost revenue is gone before a denial ever happens.
The four points where RTM billing breaks down:
Platform to EMR. The RTM platform generates a billable code, but it never becomes a charge in the EMR — because there's no integration, or the integration drops codes, maps them incorrectly, or relies on manual re-entry.
EMR to clearinghouse. The charge exists but never reaches the clearinghouse on a clean claim — it sits in an unworked charge-review queue, gets stripped by a rule that doesn't recognize the RTM code set, or goes out missing required modifiers (GP/GO/GN, and CQ/CO where a PTA or OTA is involved). Or the patient was discharged. Just a litany of ways it could go wrong.
Clearinghouse to payer. The claim rejects at the front-end edit level before the payer sees it — wrong place of service, missing diagnosis linkage, mismatched units. These are rejections, not denials, and they sit unworked because they never enter the denial queue the billing team monitors.
Payer adjudication. Only what survives all three handoffs can deny on the merits. By the time a practice reviews its RTM "denial rate," it's measuring the small fraction that made it through — not the larger volume that never got counted.
The result: a practice can generate RTM codes correctly every month and collect on a fraction of them, with no single point of failure to blame. The leakage is spread across four system boundaries, which is why it's nearly invisible without instrumentation at each step.
In practice, the best practices using SaRA (and not on our In-House Billing program) are between 80%-85% Claim generated in SaRA to Payer Adjudication. Most are in the 60%-75% range. With some uniquely rare exceptions as low as 10%.
What Are the RTM CPT Codes for 2026?
The 2026 RTM code set has eight codes spanning setup, device supply, and treatment management, with three new codes that lower the old all-or-nothing thresholds. The table below outlines the core requirements and national-average reimbursement structure for MSK care.
The key 2026 change: the old "you hit 15 days, you get nothing" cliff is gone. 98985 now captures partial-month device supply (2–15 days), and 98979 captures shorter management windows (first 10 minutes). But those codes only generate revenue if your billing pipeline actually carries them through to the payer.
Why Don't These Codes Make It Through the Pipeline?
Codes fail to reach the payer because the RTM code set is newer than most billing infrastructure, and each system in the chain has to recognize, carry, and correctly format codes it wasn't originally built for. The breakdowns are operational, not clinical — the work gets done, but the billing trail starts or breaks somewhere in the handoff.
Three structural reasons the pipeline leaks:
Modifier complexity. RTM codes furnished by therapists require GP/GO/GN, and the de minimis codes (98975, 98979, 98980, 98981) require CQ/CO when a PTA or OTA is involved. A code submitted without its required modifier rejects or denies.
Episode vs. calendar-month mismatch. Device supply codes are billed per 30-day episode; treatment management codes are billed per calendar month. These windows don't align, and billing systems built around the calendar month routinely miscount device-supply eligibility.
Rejections that never enter the denial queue. Front-end clearinghouse rejections aren't denials and often aren't surfaced to the billing team at all, so the revenue is lost without anyone ever seeing a claim.
How Do You Close the Gaps?
You close the RTM revenue gaps by instrumenting every handoff — so that each code generated in the platform is tracked all the way to payment, not just to creation. The point of a purpose-built RTM platform is to make sure the code survives the whole pipeline, not just that it gets calculated correctly.
SaRA Health was built to close exactly these gaps. Instead of generating a code and hoping it lands, SaRA tracks each code across the four handoffs above:
Platform to EMR: Clinicians sign the RTM note(s) within the SaRA platform, and the EMR is skipped altogether! No more waiting until the next visit or the mental gymnastics of writing a note to be in the past.
Threshold capture: SaRA tracks transmission days continuously and surfaces every billable scenario — including 98985-eligible patients (2–15 days) who used to fall below the 16-day cliff.
Management time and interactive communication: SaRA logs cumulative clinical minutes and the required real-time interactive communication, documented with date and method, so treatment management codes survive an audit.
Working Denials: SaRA's In-House Billing team works your RTM denials for you, so you focus on delivering amazing clinical value and we will take care of the rest.
Is the SaRA Health platform a Software as a Medical Device (SaMD)?
Yes. SaRA Health was reviewed by the FDA and recognized as a Software as a Medical Device (SaMD) under FDA enforcement discretion per a 513g request.
Frequently Asked Questions
Why do RTM claims get denied most often?
The payer does not pay or does not KNOW they pay. We see everyday payers denying the RTM codes, despite these same codes being expressly covered in the public medical policies. A denial to us is the start of a conversation, not the end.
Can I bill CPT 98977 and CPT 98985 in the same 30-day period?
No. They're mutually exclusive. Bill 98977 if the patient transmits data 16 or more days, or 98985 if they transmit 2–15 days — never both for the same patient in the same 30-day period.
Does RTM billing require interactive communication with the patient?
Yes and No. The treatment management codes (98979, 98980, 98981) require at least one real-time interactive communication — a phone call or video — per calendar month. Secure messages and voicemails alone don't qualify. The Device Supply (or Engage codes as we call the at SaRA) do NOT require an interactive communication.
Is there an add-on code for 98979?
No. 98981 (each additional 20 minutes) can only be added to 98980. There is no add-on for the 10-minute base code 98979. Once management time reaches 20 minutes, bill 98980 as the base instead.
Are device supply and treatment management billed on the same schedule?
No. Device supply codes (98977, 98985) are billed per 30-day episode of care; treatment management codes (98979, 98980, 98981) are billed per calendar month. These periods may not align, which is a common source of miscounted claims.
See It Work
Stop letting handoffs between systems drain revenue your team already earned. Book a live demo to see how SaRA tracks every RTM code from generation to payment across the full 2026 code set.
